Key Takeaways
- Up to 95% of autistic adults camouflage or mask their autistic traits, increasing the risk of anxiety, depression, autistic burnout and identity loss.
- Autistic people experience significant health inequalities, including poorer access to healthcare, more unmet health needs and worse health outcomes, often driven by communication barriers associated with the Double Empathy Problem.
- Autistic people communicate as effectively with other autistic people as non-autistic people do with each other. Research shows communication breakdowns occur primarily in mixed autistic/non-autistic interactions – not because autistic people lack empathy.
- Nearly 90% of non-autistic people form less favourable first impressions of autistic people within seconds, contributing to social exclusion, diagnostic delays and increased pressure to mask.
- Mental health difficulties are significantly more common in autistic people, with research showing approximately 4× higher rates of depression and 40–50% experiencing clinically significant anxiety, highlighting the importance of neurodiversity-affirming health and social care.
A large population-based study found that autistic people have a significantly shorter average life expectancy than the general population. The researchers estimated an average lifespan of 54 years for autistic people, compared with 70 years for non-autistic people-a difference of approximately 16 years.
While research into autism has expanded considerably over the past decade, widespread misconceptions about autistic communication, empathy and behaviour remain deeply embedded across society. These misunderstandings often influence how support is delivered, how needs are recognised, and how autistic people experience education, healthcare, employment and relationships throughout their lives.
Based on our daily experiences supporting autistic people and their families, we have repeatedly observed a gap between what research increasingly tells us about autism and how autistic people continue to be understood and supported in practice. This article was written to bridge that gap by exploring two concepts that are reshaping our understanding of autistic experiences: the Double Empathy Problem and autism masking, together with their wider implications for health, wellbeing and inclusion.
The Exhaustion of “Fitting In”
Many autistic people spend a significant part of their time managing how they are perceived.
Imagine spending every day calculating how much of yourself is safe to show. For many autistic people, fitting in means constantly adjusting behaviour, communication, facial expressions and reactions to meet expectations that were never designed with neurodiversity in mind. The result is often not greater acceptance, but chronic exhaustion that quietly affects mental health, confidence and overall quality of life.
Compared with the neurotypical population, autistic people are 3.3 times more likely to experience digestive disorders, 3.5 times more likely to develop endocrine diseases, and 7.5 times more likely to have conditions affecting the nervous system.
The ‘problem’ doesn’t end here. Very often, distress can be mistaken for non-compliance, shutdowns interpreted as a lack of engagement, or communication differences seen as a lack of insight or capacity. An autistic person who avoids eye contact may be perceived as disengaged; someone experiencing sensory overload may be viewed as uncooperative; while a person who struggles to describe pain in conventional ways may leave without receiving appropriate assessment or treatment.
As a result, many autistic people leave appointments feeling unheard, delay seeking help in the future, or experience healthcare as another environment where they are expected to adapt, rather than one that adapts to them.
The Double Empathy Problem: It’s a Two-Way Street
For decades, autism has been understood through a framework that measures autistic people against neurotypical social norms. Differences in communication, emotional expression and social interaction have often been interpreted as deficits, creating the expectation that autistic people should adapt, camouflage their natural behaviours and learn to communicate in ways that feel more familiar to others.
As a result, the responsibility for successful interactions has historically been placed almost entirely on the autistic person, while little attention has been given to whether health professionals, educators, employers or society should adapt in return.
The Double Empathy Problem challenges this assumption by recognising that misunderstandings arise from differences between people, not from deficits within one person. Empathy is reciprocal. Just as autistic people may struggle to interpret neurotypical communication styles, neurotypical people can equally misunderstand autistic ways of thinking, expressing emotions and interacting with others.
Research published over the past decade has consistently found that autistic adults often communicate more effectively and develop stronger mutual understanding when interacting with other autistic adults. Studies have reported higher levels of rapport, empathy and communication success in autistic-autistic interactions than in conversations between autistic and neurotypical people, supporting the idea that communication differences are reciprocal rather than one-sided.
More recently, a 2025 systematic review of 52 studies reinforced these findings. The review concluded that autistic people generally report more positive communication experiences and interpersonal relationships with other autistic individuals. These interactions were also associated with better wellbeing and improved quality of life across a range of social and personal outcomes.
Recognising this shared responsibility shifts the conversation away from “fixing” autistic people and towards creating environments where both sides make genuine efforts to understand one another, leading to more respectful relationships, better support and more equal access to care.
For example, an autistic person may communicate honestly and directly, while a neurotypical person interprets that communication as rude or lacking empathy. At the same time, the autistic person may find indirect language, implied meanings or non-verbal cues confusing or unclear. Both people leave the conversation feeling misunderstood, even though neither intended to communicate poorly.
Research suggests that autistic people often find it easier to understand one another’s perspectives, intentions and ways of communicating than non-autistic people do, reflecting a distinct pattern of mutual understanding between autistic peers.
The Biological Toll of Autism Masking
It often develops as an automatic survival response after repeated experiences of rejection, bullying, punishment or being misunderstood. Over time, the brain learns that hiding natural autistic traits may reduce conflict or increase acceptance, making masking an unconscious protective strategy rather than a freely chosen behaviour.
Research into the biology of autism and emerging work in molecular autism suggests that chronic masking can place significant stress on the body’s nervous system. Constantly monitoring facial expressions, suppressing stimming, forcing eye contact or rehearsing conversations requires sustained cognitive and emotional effort. This prolonged state of vigilance may contribute to elevated stress hormones, nervous system dysregulation, fatigue, anxiety and autistic burnout.
The distinction is important: adapting to different social situations can be a healthy, voluntary skill that everyone uses, but masking driven by fear of negative consequences is fundamentally different. It is not simply “pretending”; it is often an involuntary response developed to stay emotionally or physically safe in environments that do not understand autistic communication and behaviour.

How Double Empathy and Autism Masking Interact
The Double Empathy Problem and autism masking are closely connected. When autistic people repeatedly experience misunderstanding, misinterpretation or social rejection, many begin masking their natural communication style to reduce the risk of rejection and fit into environments that were not designed with autistic ways of thinking and interacting in mind. Over time, masking can appear to “solve” communication differences on the surface, but it often hides genuine needs while placing the emotional and cognitive burden almost entirely on the autistic person. This can delay an autism diagnosis, contribute to anxiety and burnout, and affect both mental and physical health through prolonged stress.
For the autistic community, this creates a cycle that can be difficult to break:
- Misunderstanding leads to pressure to mask.
- Masking makes autism less visible to others.
- Hidden needs are overlooked or dismissed.
- Support is delayed or inappropriate.
- Long-term stress increases the risk of autistic burnout, anxiety, depression and physical health problems such as chronic fatigue, sleep difficulties, headaches or gastrointestinal issues.
For example: An autistic employee may force themselves to maintain eye contact, suppress stimming, rehearse conversations and hide sensory overwhelm throughout the workday because these behaviours are viewed as “more professional.” Colleagues may see someone who appears to be coping well, while the person returns home completely exhausted, experiences frequent migraines, struggles to sleep and eventually reaches autistic burnout. The communication breakdown has not disappeared -it has simply become invisible because the autistic person is carrying almost all of the effort.
When Misunderstanding Leads to Masking
Many autistic people describe masking as something they learned, not something they chose. It often begins after countless moments of being corrected, laughed at, excluded or told that the way they communicate is “wrong.” Rather than recognising communication as a two-way process, society has traditionally expected autistic people to do all of the adapting. For many, masking becomes the price of being accepted, even when that acceptance comes at the expense of their wellbeing.
Why Masking Doesn’t Actually “Fix” the Gap
Masking may help an autistic person avoid standing out, but it does not solve the underlying communication differences between autistic and non-autistic people. It can make interactions appear smoother on the surface while hiding confusion, stress or unmet needs underneath. The expectations remain the same, the misunderstandings continue, and the effort required to maintain the mask often grows over time. Instead of creating genuine understanding, masking can make it harder for others to recognise when an autistic person needs support or is struggling.
True communication improves when both autistic and non-autistic people make an effort to understand each other’s perspectives. This is the central idea behind the Double Empathy Problem: communication is a shared responsibility, not something that rests on one person alone. When workplaces, schools, healthcare services and communities become more accepting of different communication styles, there is less pressure to mask, conversations become more authentic, and relationships are built on understanding rather than performance.
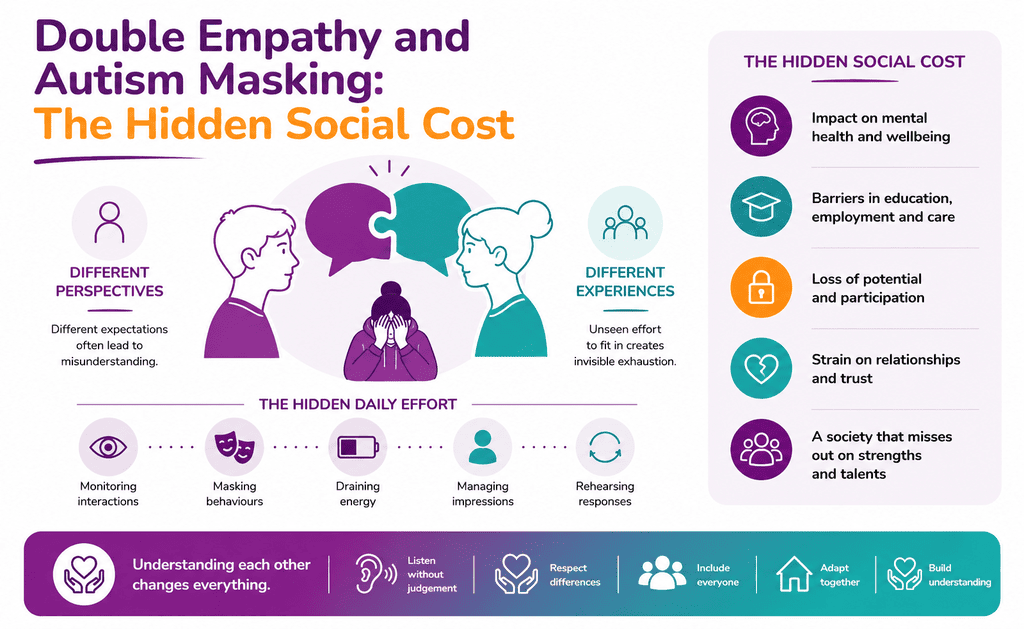
The Hidden Social Cost
Autism is often discussed in terms of communication differences, but the wider social consequences receive far less attention. When autistic people are expected to constantly adapt to environments that do not understand or accommodate their needs, the effects can accumulate over years. Social exclusion, delayed healthcare access, reduced opportunities and ongoing pressure to fit in can all affect a person’s mental wellbeing, making the real impact of autism as much about society’s response as autism itself.
Strained Relationships
The consequences of misunderstanding are not limited to awkward conversations. An autistic parent may be judged as uninterested during school meetings because they communicate differently under stress. A young autistic adult may lose friendships after repeatedly declining overwhelming social gatherings, while colleagues may wrongly interpret sensory overload or shutdown as a lack of motivation or professionalism.
In healthcare settings, communication differences can even influence clinical decisions when emotional distress is expressed in unexpected ways. These experiences demonstrate how communication difficulties and unmet expectations between autistic people and non autistic peers can gradually affect relationships, employment, healthcare access and long-term mental wellbeing.
Workplace Challenges
Despite having valuable skills and qualifications, many autistic people face significant barriers to employment because workplaces continue to prioritise neurotypical ways of communicating, interviewing and collaborating. Success is often measured by confidence in social situations rather than job performance, leaving many autistic employees under pressure to mask their differences simply to fit in.
In the UK, only around one in three autistic adults (34%) are employed, compared with more than four in five non-disabled adults (82%). At the same time, 77% of unemployed autistic adults would welcome the chance to work, suggesting that the problem is not ability or motivation, but unequal access to employment opportunities.
Barriers in Education and Care Settings
The Double Empathy Problem can have serious consequences in education, health, and social care because misunderstandings often influence the support autistic people receive. A child may be excluded from school instead of being given appropriate adjustments, while an autistic adult’s needs may remain unrecognised until they reach crisis.
These outcomes are rarely the result of autism itself, but of systems that fail to recognise and respond to different ways of communicating. Recent UK research found that one in six autistic pupils (16.2%) had not attended school at all since the start of the academic year, with 62% reporting mental health difficulties as the main reason for their absence.
Why Masking is More Common in Certain Groups
Autism masking is not equally common across all autistic people. Research suggests it is more frequently reported by autistic women and girls, people diagnosed later in life, and those who have repeatedly experienced misunderstanding or social exclusion.
Many develop masking while trying to navigate communication challenges between autistic and neurotypical people, particularly in environments where autistic differences are viewed as social deficits rather than differences in communication. The greater the pressure to meet neurotypical expectations, the more likely a person is to rely on masking as a way to avoid negative judgement or rejection.
Late-Diagnosed Adults
Before receiving an autism in adulthood diagnosis, many people spend years trying to understand why they never seem to fit in. They often believe they need to work harder to socialise, communicate or behave like everyone else, without realising they are autistic. As they repeatedly adapt to neurotypical expectations, masking becomes a way of avoiding rejection and navigating everyday life. By the time they receive a diagnosis, many realise they have been masking for years, and experiences that once felt confusing finally begin to make sense.
Reducing the Need for Masking
Reducing the need for masking begins with changing the expectations placed on autistic people. For decades, many autistic children and adults have been taught-directly or indirectly-that success depends on suppressing autistic behaviours and adopting neurotypical social norms. This constant self-monitoring comes at a significant emotional cost.
When schools, workplaces, healthcare providers and communities recognise autistic characteristics as natural forms of neurodiversity rather than behaviours that need correcting, the pressure to hide them gradually decreases. Acceptance, flexible communication, sensory accommodations and genuine understanding create spaces where autistic people can participate authentically, without sacrificing their identity simply to fit in.
Unmasking can reduce chronic stress, anxiety and emotional exhaustion by allowing autistic people to stop constantly monitoring their behaviour.
The Double Empathy Problem in Health and Social Care
Many autistic people do not struggle to access health and social care because they are unwilling to engage, but because communication differences are often misunderstood by healthcare providers and support services. The Double Empathy Problem helps explain why appointments, assessments and care planning can break down when autistic communication styles are interpreted through neurotypical expectations.
A person who avoids eye contact, needs extra time to process information or communicates in a direct way may be incorrectly viewed as uncooperative, disengaged or lacking insight. These misunderstandings can delay access to appropriate services, reduce trust in professionals and leave autistic people without the support they need.
Recognising communication as a two-way responsibility allows health and social care professionals to adapt their approach, leading to more accurate assessments, stronger therapeutic relationships and more equitable access to services.
The “Double Empathy” Bridge Should Be Built From Both Sides
The Double Empathy Problem challenges the long-standing belief that autistic people alone are responsible for overcoming communication barriers. Research suggests that the double empathy gap arises because autistic and non-autistic communication styles are based on different ways of experiencing, processing and expressing information. Expecting autistic people to carry the entire responsibility for successful interactions reinforces misunderstanding rather than improving communication.
Closing this gap requires reciprocal adaptation, where both autistic and non-autistic people recognise communication differences, adjust their expectations and develop shared understanding. When responsibility is shared instead of placed on one person, communication becomes more accurate, relationships become stronger, and autistic people are less likely to feel pressured to mask who they are.
Supporting the “Unmasked” Self with Catalyst Care Group
At Catalyst Care Group, we believe autistic people should never feel they have to hide who they are to receive the right support. Our experienced multidisciplinary team – including Positive Behaviour Support (PBS) practitioners, Community Psychiatric Nurses (CPNs) and Community Transition specialists-works alongside each person to understand their communication, sensory needs, strengths and aspirations. By adapting support to the person, rather than expecting the person to adapt to the service, we help create environments where authenticity, choice and independence can flourish.
Through evidence-based, trauma-informed and person-centred approaches, we focus on improving quality of life, reducing distress and supporting meaningful participation in everyday life. Whether someone is transitioning from hospital, experiencing a mental health crisis or receiving long-term community support, our goal is the same: to provide compassionate care that empowers people to live as themselves, not as the version they feel expected to be.
Need personalised autism support? Contact us today.