Under the Mental Capacity Act 2005 (MCA) in the UK, a person may be regarded as deprived of their liberty when they are subject to ongoing supervision and control, are not able to leave their care setting (such as a hospital or care home), and do not have the capacity (at the time of assessment) to agree to these arrangements.
For Deprivation of Liberty Safeguards (DoLS) to apply, both elements – continuous supervision and a lack of freedom to leave – need to be present.
Below is a brief overview of Deprivation of Liberty Safeguards (DoLS), designed to help families understand when these safeguards apply, how decisions are authorised, and how dignity, choice, and legal protections should be upheld when liberty is restricted.
What Does “Deprived of Liberty” Mean in Social and Health Care?
In health and social care, being “deprived of liberty” means a person is being looked after in a way they haven’t been able to agree to, because they may not have the capacity to make that decision. They are closely supported and supervised, and they’re not able to leave the place where they are living or receiving care.
This can sometimes involve things like locked doors, close monitoring, or physical support, all with the purpose of keeping them safe. The idea behind this legal framework is to protect people who need care, while still respecting their dignity, rights, and overall well-being.
Key Elements of Deprivation of Liberty
A key legal judgment from the UK Supreme Court introduced what is often called the “acid test.” It helps to understand when someone’s care arrangements go beyond support and begin to limit their liberty.
A person may be considered deprived of their liberty when all three of the following are present:
Lack of Capacity (based on a current mental capacity assessment)
The person is not able to understand or agree to the care or treatment being provided at the time of assessment. This means decisions are being made on their behalf because they are unable to give informed consent.
Continuous Supervision and Control
Support is not occasional or light-touch. Instead, there is ongoing oversight of daily life – such as where the person goes, what they do, and how they are supported. This level of monitoring can be in place to keep someone safe, but it still represents a high degree of control.
Not Free to Leave
The person is not able to leave their care setting whenever they choose. This doesn’t only mean physically locked doors – it also includes situations where staff would step in to stop them leaving if they tried, even if that is done with good intentions.
What matters here is not whether the care feels kind or whether the setting is comfortable. Even in supportive environments, if these three elements are present together, the law may recognise this as a deprivation of liberty. This definition exists to protect people – making sure that when someone’s freedom is restricted, it is properly assessed, authorised, and regularly reviewed, rather than happening unnoticed.
The Legal Framework Behind Deprivation of Liberty
When someone’s freedom is being limited in care, there must be a clear and lawful reason for it. All of this is supported by a legal framework that makes sure any restriction is properly justified, formally authorised, and carried out under strict rules.
Note: Any situation where a person is deprived of their liberty must be clearly identified, legally authorised, and regularly reviewed to ensure it remains necessary and appropriate.
This framework is there to protect people’s human rights, ensuring that decisions about their freedom are respectful, proportionate, and never taken lightly.
Below are the main laws that guide how deprivation of liberty is understood and applied in practice.
Mental Capacity Act (MCA) 2005
The Mental Capacity Act 2005 is a law in England and Wales that supports and protects people aged 16 and over who may find it difficult to make their own decisions because of illness, injury, or disability. It sets out how decisions should be approached in a way that respects people’s rights, dignity, and independence.
At its heart, the Act is built on five guiding principles that shape how care and support are provided:
- Start by assuming capacity – every person should be treated as able to make their own decisions unless it is clearly shown otherwise.
- Offer the right support – people should be given as much help as possible to understand and make their own choices.
- Respect unwise decisions – making a decision others may disagree with does not mean a person lacks capacity.
- Act in best interests – if a person cannot make a decision, any action taken must reflect what is best for them.
- Choose the least restrictive option – any support or intervention should interfere as little as possible with the person’s freedom and rights.
What does “lack of capacity” mean?
A person is considered to lack capacity if, at the time a decision needs to be made, they are unable to make that decision because of an impairment or disturbance in how their mind or brain works.
Deprivation of Liberty Safeguards (DoLS)
Deprivation of Liberty Safeguards (DoLS) are legal protections used in England and Wales to support people who may not have the mental capacity to agree to their care arrangements, particularly in hospitals or care homes.
They are there to make sure that if someone’s freedom is being restricted, it is done lawfully, only when necessary, and always in a way that considers their wellbeing and rights.
DoLS also help prevent situations where someone is effectively detained without proper oversight. Any such arrangement must be formally authorised by a Local Authority, helping to ensure accountability and respect for human rights. Over time, DoLS will be replaced by the Liberty Protection Safeguards (LPS).
Key aspects of DoLS
- Who it applies to
DoLS apply to adults aged 18 and over who are in hospitals or care homes, where they are under continuous supervision and are not free to leave. - Authorisation process
Care homes or hospitals must request approval from the Local Authority before putting these arrangements in place. - Assessments
Before authorisation, a series of assessments are carried out to understand the person’s situation. These include looking at mental capacity, mental health, age, and whether the arrangements are in the person’s best interests. This process involves trained professionals, including a Best Interests Assessor and a doctor. - Representation and support
The person is supported by a Relevant Person’s Representative (RPR). This can be a family member or an advocate, helping make sure the person’s voice is heard and that decisions can be challenged if needed. - Ongoing oversight
DoLS are not a one-time decision. Arrangements are regularly reviewed to ensure they remain appropriate and lawful.
What might count as a deprivation of liberty?
A person may be considered deprived of their liberty when restrictions go beyond what would normally be expected in care. This can include situations such as:
- Being prevented from leaving the setting
- Close or constant supervision
- Limited or controlled contact with family or others
- Use of medication or restrictions that go beyond standard care practices
Human Rights Act 1998 (Article 5)
Article 5 of the Human Rights Act 1998 protects the right to freedom and personal safety.
It means a person’s freedom cannot be taken away unless there is a clear legal reason, and the proper legal process has been followed.
What this means:
If someone is detained, they have the right to:
- be told why this is happening, in a way they understand
- be brought before a judge without delay
- challenge the detention in court
- have their case dealt with within a reasonable time, or be released
- receive compensation if the detention is unlawful
When this can happen:
The law allows a person’s freedom to be restricted in certain situations, such as:
- after a criminal conviction or when there is reasonable suspicion of a crime
- if a court order has not been followed
- for health and safety reasons, including some mental health situations
- in cases involving children and legal supervision
- for immigration purposes
Note:
Any restriction of liberty must always be lawful, clearly justified, and carried out in a way that respects the person’s rights.
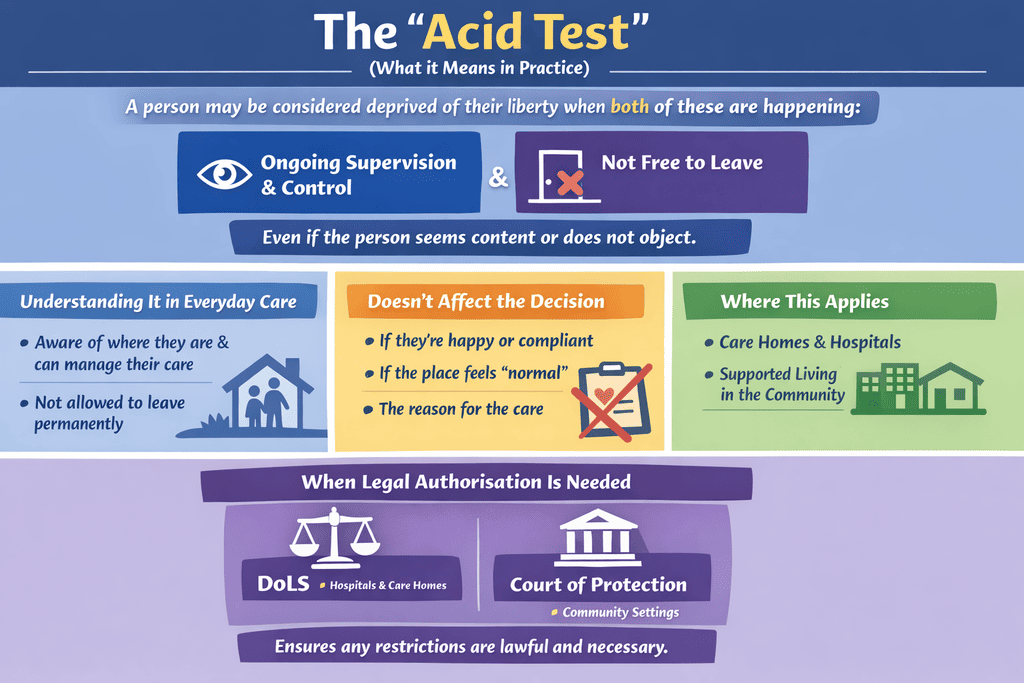
The “Acid Test”: How the Courts Define Deprivation of Liberty
The “acid test” comes from a UK Supreme Court decision and gives a simple way to recognise when someone’s freedom may be restricted.
A person may be considered deprived of their liberty when both of these are happening at the same time:
- They are under ongoing supervision and control
- They are not free to leave where they are living
This applies even if the person seems content or does not object. If the person is not able to agree to these arrangements themselves, then legal authorisation is required under DoLS.
How to Understand It in Everyday Care
Ongoing supervision and control
This does not mean someone is watched every second. It means carers or staff are consistently aware of where the person is, what they are doing, and are able to step in or make decisions about their care and movement when needed.
Not free to leave
This means the person would not be allowed to leave permanently. If they tried, steps would be taken to stop them or bring them back.
What Does Not Change the Decision
The Supreme Court made it clear that some things might feel important, but do not affect whether someone is deprived of their liberty:
- Whether the person appears happy or agrees with the situation
- Whether the setting feels comfortable or “normal”
- The reason behind the care or support arrangements
Where This Applies
The acid test can apply in different settings, including:
- Care homes and hospitals
- Supported living or care in the community
As long as care arrangements are organised or overseen by the state, the same principles apply.
When Legal Authorisation Is Needed
If a person cannot consent to their care and both parts of the acid test are met, the situation must be formally authorised.
This is done through:
- DoLS (for hospitals and care homes)
- Court of Protection (for community settings)
This process makes sure that any restrictions are lawful, necessary, and in line with the person’s rights and well-being.
Common Situations Where Deprivation of Liberty Occurs
Deprivation of liberty does not only happen in one type of setting. It can arise in different care environments whenever a person is closely supervised, not free to leave, and does not have the capacity to agree to those arrangements. What often matters is not the place itself, but how care is being delivered within it.
In some situations, these arrangements may be put in place for a short period – for example, through an urgent authorisation that can last for up to seven days while a full assessment is being arranged.
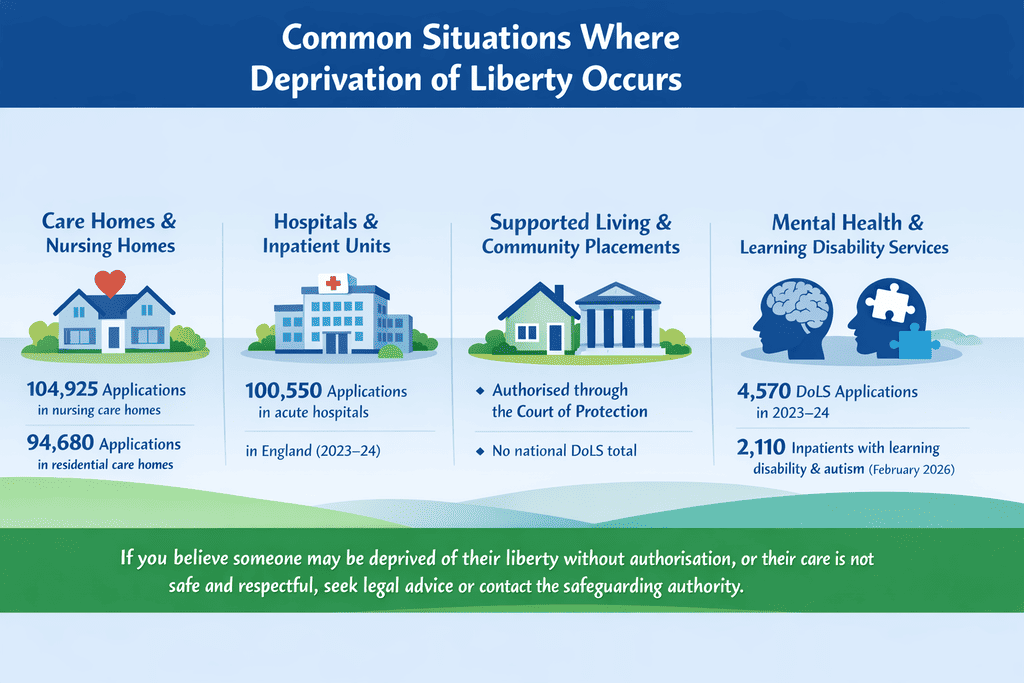
Below are some of the most common settings where this can happen, with simple examples to bring this into context:
Care homes and nursing homes
People living in care homes may have their movements closely monitored, with staff supporting most aspects of daily life. Doors may be locked, and decisions about leaving the home are often made by the care team.
Example:
A person with advanced dementia is not allowed to leave the care home alone. If they try, staff gently guide them back inside to keep them safe.
Hospitals and inpatient units
In hospital settings, especially during treatment or recovery, people may be under continuous supervision. Restrictions can be put in place to prevent harm, particularly if someone is confused or unwell.
Example:
A person recovering from surgery is closely monitored and not allowed to leave the ward due to risks to their health, even if they express a wish to go home.
Supported living and community placements
Even in more independent settings, deprivation of liberty can still occur if there is ongoing supervision and limits on freedom to leave. The environment may feel less restrictive, but the level of control remains important.
Example:
A person living in supported accommodation is accompanied by staff at all times in the community and would be prevented from leaving the placement if they tried to move elsewhere.
Mental health and learning disability services
People receiving support in these services may experience restrictions as part of managing risks, behaviours, or health needs. This can include close observation, structured routines, or limits on movement.
Example:
A person in a specialist unit is under constant supervision, with staff making decisions about where they can go and when, to reduce risk linked to their mental health needs.
If you suspect that someone may be deprived of their liberty without proper legal authorisation, or that their care is not being carried out in a safe and respectful way, it is important to seek legal advice or raise this with the relevant safeguarding authority.
How Restraint Can Lead to Deprivation of Liberty
Restraint can become a deprivation of liberty when it goes beyond a one-off or short-term safety measure and turns into something ongoing that limits a person’s freedom in a significant way. This might happen when physical restraint, medication, locked environments, or constant supervision are used regularly to control movement or behaviour, especially when the person cannot consent to these arrangements.
Over time, these restrictions can mean the person is no longer free to leave or make choices about their daily life, even if the intention is to keep them safe. When restraint reaches this level, it is no longer just care or support – it becomes a matter that must be clearly justified, legally authorised, and carefully reviewed to ensure the person’s rights are respected.
Everyday Care Practices That May Amount to Deprivation of Liberty
In everyday care settings, certain practices can quietly cross the line into deprivation of liberty, particularly for people living with dementia, mental health needs, or autism, who may already rely on others for support with decision-making:
- Locked doors and keypads – preventing a person from leaving freely, even if they want to
- One-to-one supervision – continuous monitoring that limits privacy and independent movement
- Restricting access to the community – not allowing someone to go out, or requiring permission and escort at all times
- Controlling routines, visitors, or communication – deciding when someone eats, sleeps, who they see, or how they stay in touch with others
While these measures are often introduced to keep people safe, they can, over time, significantly limit freedom and choice. When a person is under continuous supervision and not free to leave, and is unable to consent to these arrangements, care can move into deprivation of liberty, meaning it must be clearly justified, legally authorised, and regularly reviewed to protect their rights and independence.
Deprivation of Liberty vs Restrictive Practice
Restrictive practice and deprivation of liberty are closely related, but they are not the same. Restrictive practices are measures used to limit a person’s actions or choices, often to reduce risk or prevent harm, such as supervision, medication, or limiting access to certain spaces.
In many cases, these can be appropriate and proportionate when used for short periods and in the least restrictive way. However, when these restrictions become continuous, remove a person’s freedom to leave, and the person is unable to consent, they can reach the threshold of deprivation of liberty.
At that point, the situation is no longer just about care or safety – it requires clear legal authorisation, oversight, and regular review to ensure the person’s rights, dignity, and independence are upheld.
The Role of Capacity and Best Interests
Capacity and best interests sit at the centre of decisions about deprivation of liberty. A person must first be assessed to understand whether they can make their own decisions about care and living arrangements; if they can, their choice must be respected, even if others disagree.
If they cannot, any decision made on their behalf must be in their best interests, taking into account their wishes, feelings, values, and input from people who know them well. This also means choosing the least restrictive option possible, so that any limitations on freedom are proportionate, clearly justified, and kept under regular review.
Preventing Unnecessary Deprivation of Liberty
Preventing unnecessary deprivation of liberty begins with a simple but important question: is this restriction truly needed, or is there a less restrictive way to provide support? By focusing on each person’s abilities, preferences, and ways of communicating, care can be tailored to support safety without compromising autonomy and independence.
Simple changes – like actively involving people in their care, understanding what makes them feel comfortable, recognising what may trigger distress or unpleasant emotions, and taking a proactive approach to care that places the person at the centre of every decision-making.
Trauma-informed Practices
Trauma-informed care recognises and responds to the signs, risks, and lasting impact of trauma, helping to better understand and support the needs of people who have experienced social, physical, or emotional trauma. Many people in care, including autistic people and people with learning disabilities or mental health needs, have experienced trauma that is not always visible.
Example: A person may have had a traumatic experience in the past involving someone wearing a red shirt. Over time, the colour red or a similar shirt may become a trigger, causing distress or behaviour of concern whenever it is seen. With a trauma-informed approach, this can be recognised early, understood in context, and responded to in a way that reduces distress – helping to prevent escalation and avoid unnecessary restrictions that could lead to a deprivation of liberty.
Positive Behaviour Support (PBS)
Positive Behaviour Support (PBS) is a proactive, evidence-based way of supporting people that starts with understanding why something is happening, not just reacting to it. Instead of focusing on stopping behaviour, it looks at what a person might be trying to communicate and how their environment affects them. By helping people learn new skills and creating support that works for them, PBS makes everyday life feel more manageable, more predictable, and more respectful of who they are.
The aim of Positive Behaviour Support (PBS) is to minimise restrictive practices by taking a proactive approach to reducing behaviours of concern. It focuses on understanding the reasons behind behaviour and using personalised assessment and tailored care plans to improve quality of life, while supporting people in a way that respects their needs and everyday experiences.
What to Do If You Think Someone Is Being Deprived of Their Liberty
If there is a concern that someone may be deprived of their liberty, or a safeguarding concern, it is important to act quickly. Raise it immediately with the care home, hospital, or service providing the support. Ask simple questions – is the person free to leave, and is there legal authorisation in place (like DoLS)? If concerns remain, report it without delay to the local authority safeguarding team or an advocate so the situation can be urgently checked and the person’s rights protected.
Catalyst Care Group Provides Care in Line with the Deprivation of Liberty Safeguards and the Mental Capacity Act
At Catalyst Care Group, support is shaped around people through person-centred, integrated care grounded in a human rights approach and a clear legal framework. Using Positive Behaviour Support (PBS), proactive care, and least restrictive practices, teams work to manage crises, support smoother transitions, and reduce unnecessary hospital admissions.
As a certified PROACT-SCIPr-UK® training centre, teams are equipped with the skills and confidence to support people with behaviours of concern in a compassionate and structured way. Support is guided by a clear assessment process, including functional and intentional assessments, alongside best interests assessment to ensure decisions reflect the person’s needs, rights, and overall wellbeing.
Support plans are developed with proactive strategies, focusing on reducing reliance on reactive and restrictive interventions. Each person’s care arrangements are carefully designed and regularly reviewed to ensure they remain appropriate, least restrictive, and aligned with their rights.
To further minimise restrictions, a wide range of specialist support is available, including occupational therapy, mental health support, and multimedia approaches.
Working as a multidisciplinary team – including PBS specialists, speech and language therapists, community psychiatric nurses, and in partnership with the Restraint Reduction Network – support is coordinated and consistent. This includes:
- Functional and intentional assessments of behaviours of concern
- Evidence-based support strategies
- Regular, personalised training for support teams
- Tailored PBS plans
- Collaborative, multidisciplinary working
- Ongoing emotional support and open conversations with teams
With a clear commitment to Building the Right Support, Catalyst Care Group works alongside wider systems to find practical, least restrictive solutions – so people can receive high-quality, person-centred support within their own homes and communities.
For more information, contact us today.