Key Takeaways
- Positive Behaviour Support has moved beyond behaviour management
PBS is no longer used only to analyse and manage behaviour. Services now expect a more detailed, proactive approach to why behaviour happens, including the person’s history, environment, and unmet needs. - Trauma is more present across services than previously recognised
Many people in health and social care have experienced trauma, and this directly affects how they respond to support, routines, and change. - Behaviour is increasingly linked to past trauma and lived experience
What appears as distress, resistance, or escalation is often connected to previous experiences of harm, loss of control, or feeling unsafe. - Reactive care models have done more harm than good
Waiting for behaviour to escalate and then responding in crisis leads to repeated breakdowns, restrictive interventions, and unstable support. - This is driving the need for a more proactive approach to care
Trauma-informed PBS focuses on early understanding, recognising triggers, and putting the right support in place before distress escalates.
Positive Behaviour Support (PBS) is built on working closely with children, young people, adults and their families to improve everyday life and reduce unnecessary restrictions. It recognises that behaviours of concern are often a way of showing that something is not working or that a need has not been met. To understand the person more fully, PBS is increasingly delivered through a trauma-informed approach, taking into account past experiences of trauma, living environment, family relationships, and any time spent in institutional care.
This approach shows how PBS can be used in a practical, trauma-informed way to support healing and development in children and adults. People who need intensive care and support are often more exposed to instability, disruption, and restrictive environments, which increases the likelihood of trauma being part of their experience.
Nurseline Community Services, our trauma-informed service specialising in trauma, its impact, and recovery, has developed a comprehensive guide: Living with Trauma – How Does It Feel? Created for people who have experienced trauma, parents and families, carers, and professionals, the guide brings together practical information, real experiences, and a deeper understanding of how trauma can affect everyday life.
The guide is available to download here.
The Growing Need for Proactive Support Approaches
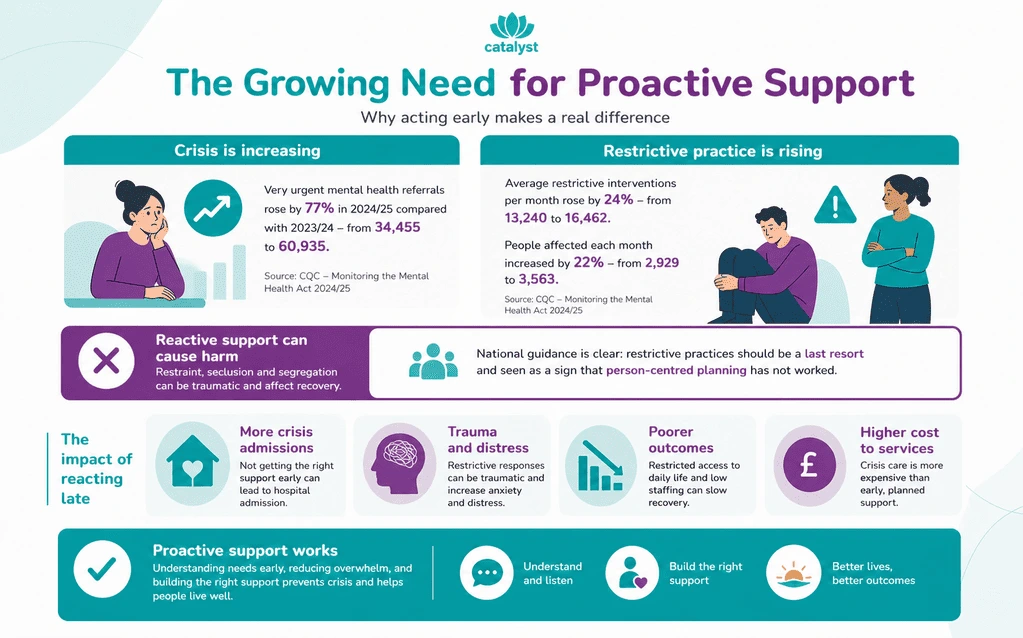
The need for proactive support approaches is growing because too many people are still only getting meaningful help when their distress has already escalated into crisis. Across England, the Care Quality Commission has warned that when people do not get the care they need at the right time, they can end up in crisis, and NHS England data cited by CQC shows that very urgent referrals to crisis services rose by 77% in 2024/25 compared with 2023/24, increasing from 34,455 to 60,935.
That rise points to a system still reacting late rather than recognising needs earlier, building the right support around the person, and preventing breakdown before hospital admission, restraint, or emergency intervention become more likely.
The negative impact of reactive support is visible in national data on restrictive practice. In its Monitoring the Mental Health Act 2024/25 report, CQC said the average number of restrictive interventions each month rose by 24% between 2023/24 and 2024/25, from 13,240 to 16,462, while the average number of people subject to restrictive interventions each month increased by 22%, from 2,929 to 3,563.
The same report also states that restrictive practices remain a particular concern for autistic people and people with a learning disability. This matters because restrictive responses are not neutral care tools. CQC has repeatedly said restraint, seclusion, and segregation can have a devastating impact and can themselves be traumatic.
For people with a learning disability and autistic people, the case for proactive support is even clearer. CQC has said that not getting the right support early on can lead to hospital admission, and that lack of community alternatives can leave people stuck in settings that are not therapeutic, sometimes for years, increasing the risk of restraint, seclusion, and segregation.
NHS England now states that care must be trauma-informed, autism-informed, and culturally competent, while its guidance on restrictive practice says the use of restrictive practices should be treated as an inherent risk factor and reflects a failure of person-centred planning. That is a strong signal from national bodies: good care cannot be built around containment alone.
The Core Components of Proactive Care
Proactive care starts by really getting to know what affects a person day to day – what causes pressure, what feels overwhelming, and what might lead to distress if it builds up. Instead of waiting for things to reach a crisis point, it focuses on noticing these patterns early, including triggers such as communication difficulties or environmental stress, so support can be adjusted in time.
Within Positive Behaviour Support (PBS), this approach is closely linked to trauma-informed practice. It recognises that past experiences often sit underneath behaviours of concern, and that both people receiving support and those providing it can be affected by trauma. When this is understood, support becomes more thoughtful, consistent, and better able to support healing, rather than simply reacting when things go wrong.
Positive Behaviour Support PBS
Positive Behaviour Support (PBS) is a proactive, evidence-based approach that starts by understanding the root causes of people’s behaviour. It is focused on teaching new skills and creating supportive environments – ensuring dignity, growth, and meaningful outcomes in all aspects of people’s lives.
At Catalyst Care Group, PBS transforms behaviour support from reactive control to proactive investment in human potential, reducing crises through trauma-informed and compassionate ethical strategies.
The aim of Positive Behaviour Support (PBS) is to minimise restrictive practices by using proactive approach to reducing behaviours of concern while improving people’s quality of life.
Behaviours of concern are identified by considering the following factors:
- Is the behaviour harming or limiting the person’s quality of life?
- Is the behaviour causing a risk of harm to the person?
- Is the behaviour causing a risk of harm to other people? Are there restrictions in the person’s life due to the specific behaviour?
All our PBS practices are founded on value-based models of care developed in cooperation with the Loddon School and the Reduction Restraint Network. Trained in PROACT-SCIPr-UK®, our team uses the person-first approach and proactive strategies to support personal growth and prevent crisis intervention.
Trauma-Informed Practice
Trauma-informed care recognises and responds to the signs, risks, and impact of trauma, helping teams better understand and support the specific needs of people who have experienced social, physical, and emotional trauma.
Trauma is the emotional shock that can follow a deeply distressing or frightening experience. It can arise after experiencing a frightening event, witnessing one, or learning that it happened to someone close.
The response becomes traumatic when it brings intense fear, helplessness, horror, or a sense of being overwhelmed beyond usual coping abilities. This can leave lasting effects on emotional regulation, psychological health, physical well-being, and social connections.
For many people in care, the impact of past trauma can increase the risk of repeated re-traumatisation unless carers are supported to recognise and respond to these effects.
A trauma-informed approach begins by asking “what has happened?” rather than “what’s wrong?”. It recognises that behaviours often develop as ways of coping, adapting, or surviving difficult experiences. With that understanding, care can move towards supporting healing, building resilience, and helping people feel safe enough to trust services while developing skills for emotional regulation and overall well-being.
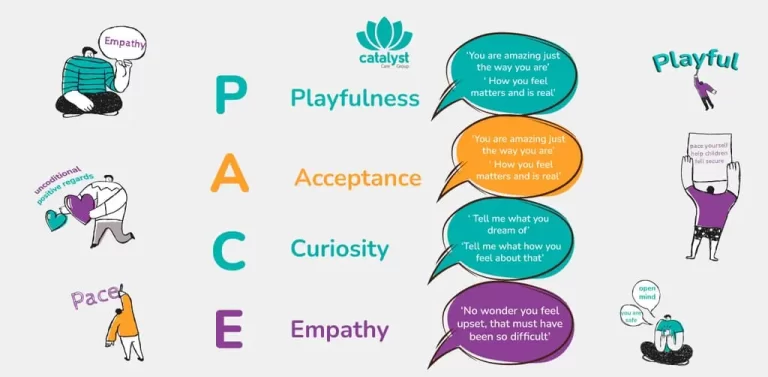
In practice, this approach is often described through four core ideas:
- Realise – understanding how trauma can affect people, as well as families, teams, and wider communities
- Recognise – being able to notice signs that someone may be responding to trauma
- Respond – shaping everyday support and environments in line with this understanding
- Resist re-traumatisation – being mindful of triggers and avoiding practices that could cause further distress, including restrictive approaches
What is Trauma-Informed PBS?
The aim of Positive Behaviour Support is to improve the quality of life. It uses behavioural approaches to understand behaviour and ensure that people’s needs are met through the team supporting them. PBS is not a single approach; other evidence-based methods can also be part of support. While it is grounded in values and behavioural understanding, it also recognises that a person’s life history and feelings matter. These experiences are central to shaping support that truly fits the person.
From experience, how often have people you’ve developed positive behaviour support plans for had a history of trauma?
Combining behavioural understanding with trauma awareness strengthens how positive behaviour support is applied in practice. For autistic people, people with learning disabilities, and others who are more likely to have experienced trauma, behaviour cannot be understood only through triggers and consequences.
Trauma can affect how stress is processed, how safe environments feel, and how people respond to support, including difficulties with emotional regulation, attention, and impulse control. This means behaviour is often shaped by both present conditions and past experiences.
When both are considered together, support becomes more consistent and responsive, focusing on reducing distress, increasing predictability, and creating environments where people feel safe enough not to rely on behaviour as a way of coping or communicating.
- What might feel overwhelming or unsafe for this person?
- What truly matters to them in their day-to-day life?
- What do their routines and familiar patterns show about what they value?
- What does a good day look like, and what tends to make a day difficult? What is working well, and what is not?
- How well are the people supporting them matched to their needs and preferences?
- What choices are available to them, and how are these supported?
- What would help them experience a better quality of life?
The Impact of Trauma on Behaviour
Trauma has a measurable and lasting impact on how people respond to the world around them. Large-scale studies on Adverse Childhood Experiences (ACE) show a clear link between early trauma and later emotional regulation difficulties, heightened stress responses, and increased likelihood of behaviours that challenge.
Neurological research also shows that trauma can alter how the brain processes threat, keeping people in a state of hypervigilance or shutdown, where reactions are driven by survival rather than choice.
In health and social care, this is reflected in higher rates of distress, self-injury, and crisis behaviours among people with a history of trauma – particularly for autistic people, people with learning disabilities, and people with mental health needs, who are also more likely to experience trauma in the first place. Seen in this context, behaviour is not random or purely behavioural; it is often a direct expression of past experiences, stress, and unmet need.
The Neurobiology of Trauma
When someone has lived through trauma, the brain doesn’t respond to the world in the same way anymore. It becomes more focused on staying safe than on understanding what’s actually happening. The “survival brain” steps in quickly, reacting to anything that feels even slightly threatening. This is where responses like fight, flight, freeze, or fawn come from.
They are not conscious decisions, but automatic reactions shaped by past experiences where protection was needed. For many autistic people, people with learning disabilities, and people with mental health needs, this can happen more often, especially in environments that feel overwhelming or unpredictable.
- Fight – pushing back, resisting
- Flight – avoiding or trying to leave
- Freeze – going quiet, shutting down
- Fawn – agreeing or complying to keep things safe
At the same time, the part of the brain that helps with thinking, communication, and understanding – the “learning brain” – becomes harder to access. In moments of stress, it’s not that someone doesn’t want to engage or respond, it’s that their brain is focused on getting through the moment safely. That’s why what we see as behaviour is often a response to how safe a person feels, not a reflection of what they are capable of.
Behaviour as Communication
Behaviour that is often described as “challenging” or “of concern” rarely appears without reason. For many people, especially autistic people, people with learning disabilities, or people who have experienced trauma, behaviour can be a way of communicating when words feel out of reach or unsafe.
What might be seen as aggression, withdrawal, refusal, or heightened distress can reflect something deeper – fear, confusion, sensory overwhelm, or past experiences where needs were not understood or met. In this sense, behaviour becomes protective. It is not random or attention-seeking; it is an adaptive response shaped by a need to stay safe.
This can be seen in very real, everyday moments. For example, an autistic person who is non-verbal may have had a traumatic experience involving someone wearing a red shirt. From the outside, the colour red might seem neutral or insignificant. But for that person, seeing a red shirt again can act as a powerful reminder of what happened, triggering distress or a strong behavioural response.
What looks like a sudden or unexplained reaction is, in fact, the body remembering and trying to protect itself. This kind of re-traumatisation often goes unrecognised, especially when the focus stays only on the behaviour. When behaviour is understood as communication, it becomes possible to look beyond the surface and recognise the meaning behind it – creating space for support that feels safer, more predictable, and more attuned to that person’s experience.
Common Triggers in Care Settings
Common triggers in care settings are often part of everyday routines and environments, yet their impact is easy to miss. For people who are autistic, have learning disabilities, or are living with trauma, these triggers can quickly lead to distress when they are not recognised or understood.
- Sensory input – noise, lighting, smells, or crowded spaces can become overwhelming
- Lack of choice – limited control over routines or decisions can lead to frustration or withdrawal
- Perceived power imbalances – not being listened to or involved can lead to resistance or escalation
- Environmental stressors – unfamiliar settings, unpredictability, or constant change can increase anxiety and alertness
- Communication difficulties – not being able to express needs or feeling misunderstood can lead to frustration or distress
- Changes in routine – unexpected changes can create anxiety, confusion, or resistance
- Unmet physical needs – pain, hunger, fatigue, or discomfort can quickly impact behaviour
- Trauma reminders – certain people, clothing, tones of voice, or situations can trigger strong emotional responses
- Demands and expectations – being asked to do something without preparation or at the wrong time can feel overwhelming
- Transitions – moving between activities, places, or carers can lead to anxiety or escalation
- Staff approach and interaction style – tone, pace, and body language can either reduce or increase distress
- Loss of control – being directed rather than involved can lead to withdrawal, resistance, or escalation
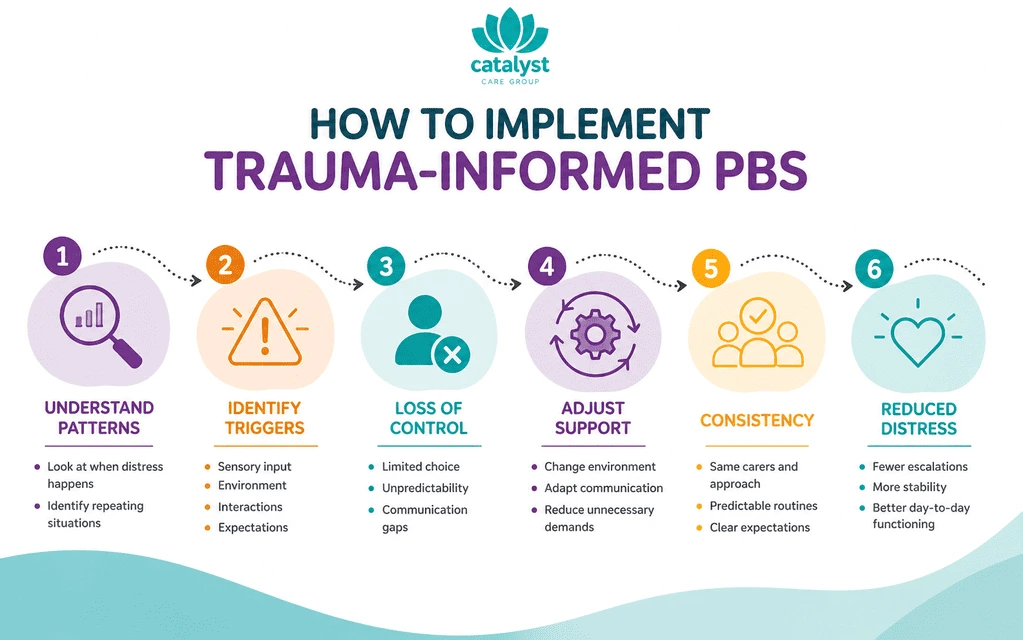
How to Implement Trauma-Informed PBS
Trauma-informed PBS focuses on understanding when and why distress happens, and what needs to change around the person to reduce it. It looks at patterns across the day, the environment, interactions, and past experiences that still affect how someone responds.
In practice, this means looking closely at patterns.
- What situations lead to distress?
- What feels unsafe, overwhelming, or out of control?
For some people, it might be sensory overload. For others, it could be certain people, environments, or even small details that connect back to past experiences. Without that understanding, support stays reactive.
Step 1: The Functional Assessment (FA) with a Trauma Lens
A functional assessment (FA) is a structured process used to understand the function of behaviour by analysing patterns across situations, interactions, and time. It combines direct observation, input from the person, family, carers, and multidisciplinary teams, along with review of history and records, to identify what consistently precedes and follows the behaviour, and what it achieves for the person.
A trauma lens adds depth by examining how earlier experiences – such as trauma, disrupted attachments, or repeated loss of control – have shaped current responses. This includes identifying “slow triggers”: learned sensitivities to specific people, environments, demands, or relational dynamics that can activate a stress response even in neutral situations.
Through this process, the assessment moves towards a clear formulation that links behaviour to both present context and past experience, allowing teams to understand the function with greater accuracy and adjust environments, interactions, and support in ways that reduce distress and increase a sense of safety and predictability.
Step 2: Designing “Capable Environments”
Designing a capable environment focuses on reducing the background stress created by sensory overload and unpredictability. Evidence shows that noise, harsh lighting, and crowded spaces can increase arousal and make it harder to stay regulated, especially for autistic people and people with trauma histories. In practice, this means making the environment calmer and easier to handle – lower noise levels, softer and consistent lighting, fewer people around at once, and clearer, predictable routines.
These changes reduce the pressure the person experiences throughout the day and make it easier to stay engaged and settled.
For example, a person who becomes distressed in a busy supported living setting during peak hours may struggle with the noise and movement around them; having access to a quieter space, fewer people around at the same time, and a calmer routine can help them feel more settled and cope better.
Step 3: Skill Teaching & Co-Regulation
Skill teaching focuses on building practical ways for a person to manage stress and communicate needs, with support from carers before expecting independence. Evidence from trauma and neurodevelopment shows that regulation is learned through repeated, supported experiences where another person helps to steady the situation in real time. Over time, these experiences build recognition of early stress and more reliable responses.
For example, a person who becomes distressed when demands change may initially rely on a carer to slow things down, explain what is happening, and guide them through the transition; with repetition, the person begins to tolerate the change better and use the same steps with less support.
Step 4: Eliminating Restrictive Practices
Eliminating restrictive practices focuses on reducing and removing interventions such as restraint and seclusion, recognising the risk of re-traumatisation and the impact these approaches can have on a person’s sense of safety and control. Evidence shows that restrictive practices can increase fear, damage trust, and reinforce distress, especially for people with past trauma.
A trauma-informed PBS approach works towards prevention by understanding triggers, adapting environments, and supporting regulation early, so situations do not escalate to the point where restriction is considered. This shifts the focus from managing behaviour in crisis to creating conditions where the person feels safer, more understood, and less likely to experience overwhelming distress in the first place.
Benefits of This Integrated Approach
When trauma awareness is integrated into Positive Behaviour Support, the focus shifts from reacting to incidents to preventing them. Support is planned around what increases stress for a person, what helps them feel safe, and how everyday environments, routines, and interactions can be adjusted to reduce the likelihood of distress in the first place. This leads to more consistent support, fewer escalations, and better long-term outcomes for both people and teams.
For The Individual
This approach improves daily experiences by reducing distress, increasing agency, and achieving positive outcomes.
- Fewer situations escalate because triggers are recognised early and reduced where possible
- Daily routines feel more predictable, which lowers anxiety and uncertainty
- More choice and involvement in decisions, even in small moments throughout the day
- Communication improves, especially for people who do not use verbal language
- Reduced reliance on restrictive practices because distress is prevented, not managed after escalation
- Stronger sense of safety with familiar carers who respond in consistent ways
- Progress happens at a pace that feels manageable, not overwhelming
For The Care Provider
- This approach leads to reduced staff turnover, fewer incidents of concern, and a more empathetic team culture.
- Reduced use of restraint and restrictive interventions
- Lower staff burnout due to less crisis-driven work
- Improved staff confidence in understanding and responding to distress
- More consistent practice across teams, reducing mixed responses
- Better retention as staff feel more supported and less overwhelmed
- Stronger collaboration across multidisciplinary teams (PBS, SALT, OT, mental health support)
Trauma-Informed PBS in the UK: The Path Forward
Across the UK, there is a growing recognition that behaviour cannot be separated from experience. Many people supported in health and social care have lived through environments that felt unsafe, unpredictable, or restrictive. Without acknowledging that, even well-intended support can unintentionally repeat patterns that increase distress.
Moving forward means building services that are designed around safety, consistency, and trust. This includes proactive approaches that identify stress early, environments that reduce overwhelm, and teams that respond in ways that do not escalate fear. It also means listening more carefully to what people show through their actions, especially when communication is not straightforward.
At its core, trauma-informed PBS is not about changing people. It is about changing the conditions around them. When people feel safe, listened to, and respected, behaviour begins to shift on its own. Not as a target, but as a natural response to being understood.
Trauma-informed PBS within Catalyst Care Group
At Catalyst Care Group, we implement trauma-informed care because many people we support have experienced trauma, including unsafe environments, repeated restrictions, loss of control, placement breakdowns, or long periods in institutional care. This understanding shapes how effective support is provided, helping teams recognise distress earlier, reduce avoidable triggers, and respond in ways that protect safety, dignity, and trust.
Through trauma-informed PBS, we combine behavioural understanding with therapeutic input to support people in a more personalised and proactive way. This means looking at what has happened in a person’s life, what may still feel unsafe for them, and what needs to change in their environment, routines, communication, and relationships. Support is shaped around each person’s experiences, strengths, and needs, with a clear focus on reducing restrictions and building stability over time.
For people with complex needs, Catalyst Care Group provides trauma-informed, multidisciplinary support that reduces distress, improves stability, and supports long-term progress in everyday life.
For more information, contact us today!